In the second part of our three-part series, Mike Davies RCVS Specialist writes about the treatment modalities used to manage canine osteoarthritis
Treatment modalities used to manage canine osteoarthritis
Clinical objectives in managing osteoarthritis should be :
Prevent or delay the onset of osteoarthritis
Breed away from anatomical traits that increase the risk of occurrence or severity of osteoarthritis
Manage pain and lameness using licensed medications (See Appendix 1), nutritional supplements and therapeutic diets
Regenerative medicine - Stem cell transplantation
Support and maintain joint movement through physiotherapy, ultrasound therapy, laser therapy, heat or cold administration, hydrotherapy (swimming, water baths)
These objectives can be achieved by:
Preventive measures
Stop breeding from lines with the worst inherited conformations that predispose to OA and use breeding programmes such as hip or elbow dysplasia schemes.
Ensure the pregnant mother and growing puppies are fed a complete and balanced diet. In a UK study (Davies and others 2017) only 6% (6/97) of wet and 38% (30/80) of dry pet foods labelled as complete were fully compliant with mineral and trace element requirements, and many foods (20-30% of all analysed) had mineral imbalance, such as not having the recommended ratio of Ca:P (between 1:1 to 2:1) which would lead to developmental skeletal disease. For example, excessive calcium intake is known to cause angular limb deformity, and osteochondrosis, and calcium deficiency causes nutritional secondary hyperthyroidism resulting in fractures and limb deformities. (Hazewinkle 1989)
Control food intake to avoid overweight and keep dogs lean with a body condition score (BCS) of under 5/9. In a lifetime study of 48 Labrador Retrievers 25% reduction in food intake delayed the onset of arthritis (based on annual radiography) by 6 years, and none of the dogs in the diet restricted group developed clinical signs of osteoarthritis (Lawler and others 2008).
Reduce body weight to relieve pain and reduce lameness.
Treatment Modalities for existing disease
There are many different strategies used in the management of osteoarthritis and a multimodal approach is usually recommended (Pye and Others 2022; Vaughan-Scott and others 1997).
Interventions include:
Anti-inflammatory drugs
Corticosteroids
Non‐steroidal anti‐inflammatory drugs (NSAIDs),
Others - Piprants
Monoclonal antibodies
Adjunctive analgesics
Structure modifying osteoarthritis drugs
Regenerative therapies.
Maintenance of joint function is important in OA because disuse can lead to atrophy and muscle wastage, so regular exercise is required, however excessive exercise and vigorous exercise is inappropriate and can increase inflammation.
In all situations, the selected treatment(s) should be safe and proven to be effective by randomised controlled studies in the species for which the intervention is intended. The use of unlicensed human medicines and unproven complementary or alternative treatments should be avoided as our clinical recommendations these days should be evidence-based, and it is unreasonable to expect owners to pay for unproven remedies.
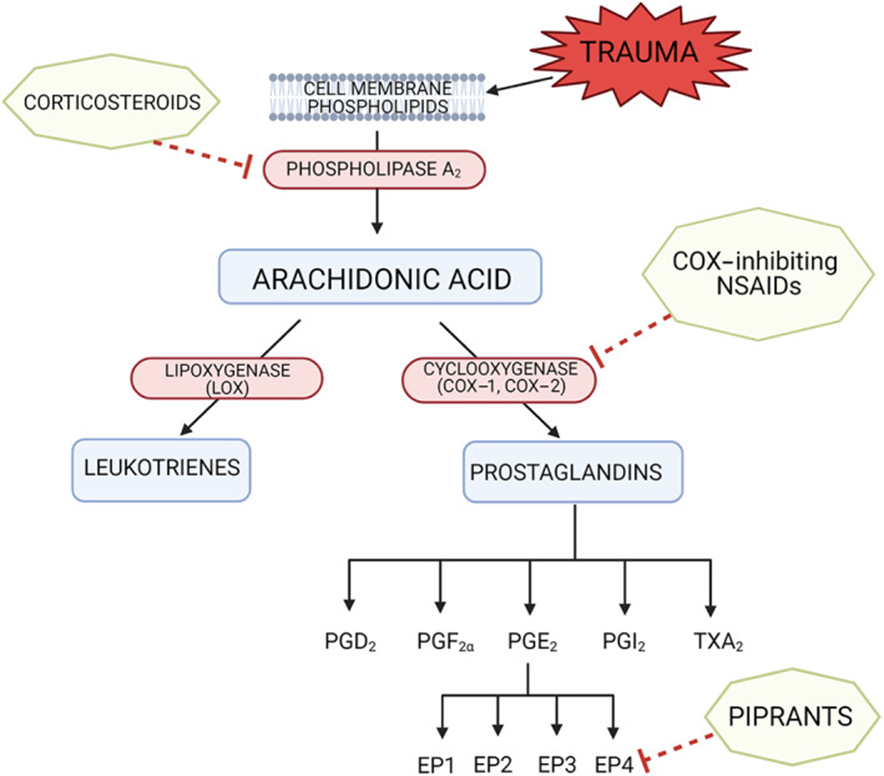
FIG 1 Targets of corticosteroids, COX‐inhibiting NSAIDs and piprants on the pathway of arachidonic acid metabolism. Corticosteroids inhibit phospholipase A2, preventing the conversion of phospholipids to arachidonic acid. NSAIDs inhibit cyclooxygenase, therefore preventing the production of prostaglandins from arachidonic acid. Piprants selectively antagonise the prostaglandin‐E2 EP4 receptor. Adapted from Monteiro & Steagall (2019)

Mike Davies, BVetMed, CertVR, CertSAO, FRCVS, graduated from the RVC in 1976. He has postgraduate qualifications in veterinary radiology and small animal orthopaedics and holds a fellowship by examination in clinical nutrition in cats and dogs.
Mike is an RCVS specialist in veterinary nutrition (small animal clinical nutrition). He has worked in academia and private practice and for several pet food manufacturers and pharmaceutical companies.
He speaks internationally on clinical nutrition and geriatrics and founded the original City and Guilds certificate in small animal nutrition, and the BVNA certificates in small animal and exotic nutrition. He runs Provet’s certificate course in clinical nutrition.
